商用空气能采暖




科技之心 阳光之星 品质之选
砥砺奋进开拓创新 坚持不懈恪守品质
家用、商用热水、冷暖需求皆可量身定制 热水系统,热水+采暖,热水+冷暖系统,灵活搭配组合 系统集成度高,安装不受场所限制 更节能、更合理、更稳定、更高效是我们的承诺

管理体系认证、暖通工程师、热利用工程师、维修工程师等技术人才 齐心协力,打造高品质工程

双节能新能源利用,清洁、高效更省钱 微电脑远程控制,系统运行稳定 水电分离更安全,全年365天稳定运行 方式灵活,可实现热水、热水+采暖、热水+冷暖多种系统搭配

免费项目现场勘查+方案报价 全程高品质一对一技术服务 售后24小时在线,无后顾之忧
致力于空气能冷暖创新技术发展 带给您高效节能安全环保的体验

近些年,在我国减煤禁煤的现行政策浪潮下,每个领域都是在不停的采取一定的有效措施革除传统式燃煤锅炉供暖方法,采用清理、环境保护的方法。在这里众多绿色能源机器设备中火爆的当属空气能热水器。我走访调查本地的蔬菜大棚发觉,许多温室大棚都早已运用上空气能取暖热泵机组。
查看详情
空气能冷暖一体机致冷采暖效果。以下属于深入分析:制冷效率:空气能冷暖一体机在制冷时,借助电磁能推动制冷压缩机工作中,运用制冷剂完成发热量迁移,并拿水来传热。这类冷却方式不但进风口适宜的温度,不会产生室内空气干燥,并且水循环系统加风盘吹风机的形式,促使使用时间长不会出现相近中央空调所带来的口干、皮肤干

1,用户的使用习惯也和取暖费使用的多少密切相关。比如有的人设定采暖温度是20℃,而有的人习惯性设置到24℃。虽然只有相差了4℃,可是室内温度每上升1℃,能源消耗就会提高10%上下,因而,需要空气能取暖花费变低,把水的温度适度的降低一些。2,不同类型的供暖尾端也是导致取暖费用高居不下缘故。空气能取暖一
工厂宿舍是员工休息的场所,良好的休息环境对提高员工的工作效率非常重要。因此,空气能采暖设备的噪音问题需要特别关注。如果宿舍周围环境过于嘈杂,员工的睡眠质量将受到影响。如果空气能采暖设备的噪音控制得当,可以使员工更加专注于工作,从而提高工作效率。首先,在购买空气能热泵时,我可以根据其材料进行选择,现在

伴随普通百姓日常生活能力的提高,大家对于家庭生活水平也拥有了更高一些的要求。对北方地区的家中来讲,冬季有采暖是一个比较常见的事。取暖的优点很多,不仅使用的时候省时省力省心省事,主要的是价格还划得来。但是相较于南方地区的很多家中来讲,冬天若想采暖,乃是一类很繁琐的新项目,并没有集中供热,务必自己买取暖

提到超低温地域,大家都会想到东北区域的雪和十分寒冷的冬季。与中国的华北平原区和中原地域对比,东北地域的冬季好像既冰冷又悠长。在东北地域,一般10月份正式进入采暖时节,直至来年5月才终止采暖。因为东北地域近期天气这般寒冷和悠长,本地取暖设备在低温下的采暖实际效果已成为我们比较关心的问题。依据综合性认知

近年来,伴随着北方地区“电代煤”工程项目的推动,空气能热水器对北方地区老百姓来说已经不再是新事物。空气能取暖热泵机组的优势有许多,例如环境保护、安全性、整洁、舒服等,但是对于老百姓来说,花费才是重要的。空气能取暖热泵采暖究竟贵吗,才是一个确定普通百姓能否接受空气能热水器变成燃煤蒸汽锅炉替代品的根本原

生产经验
生产厂房
自动化生产线
研发专利
产品认证
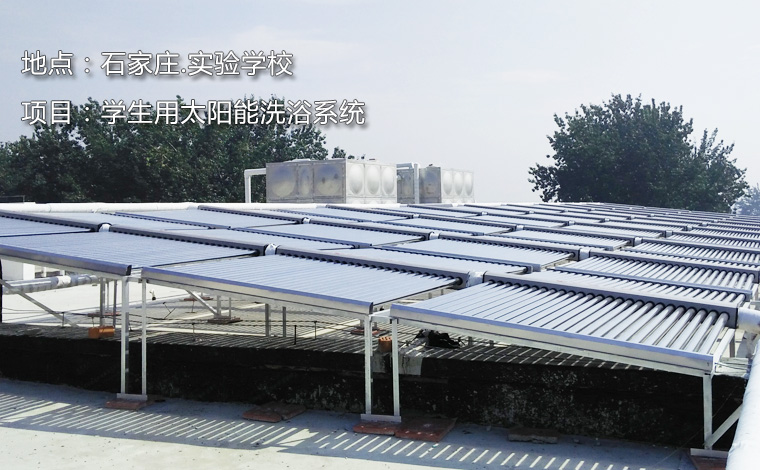
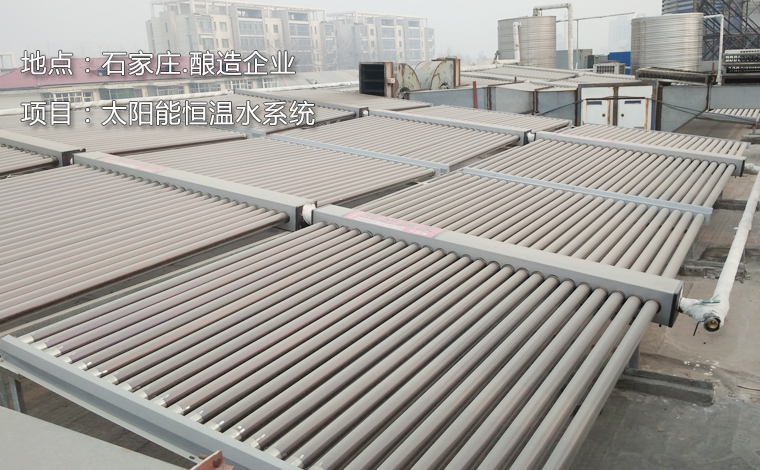
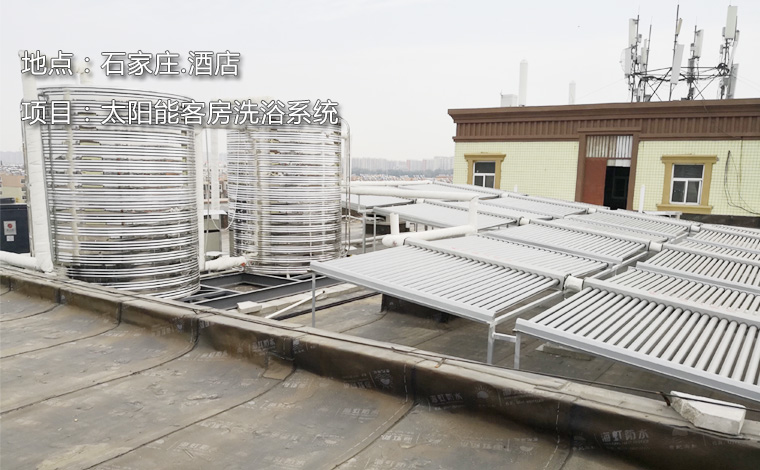
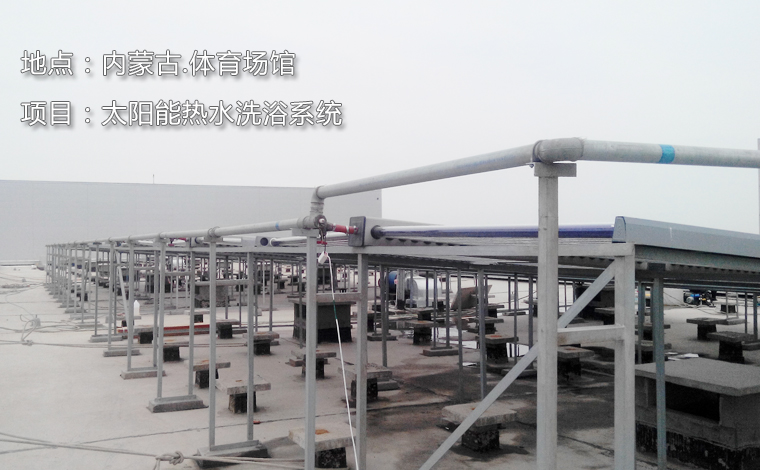
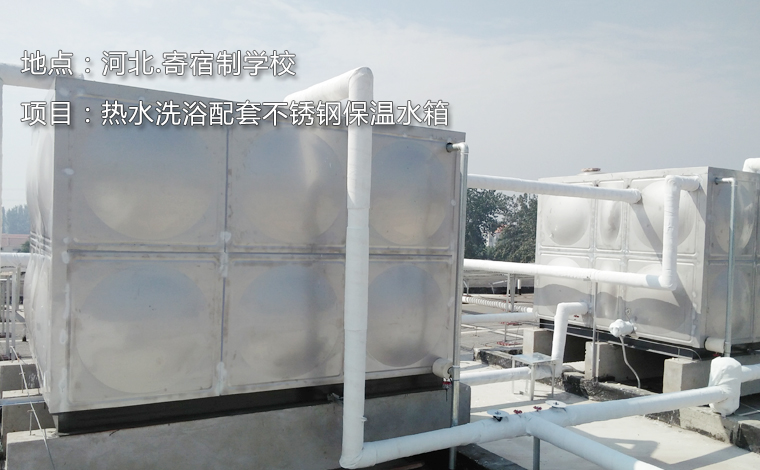
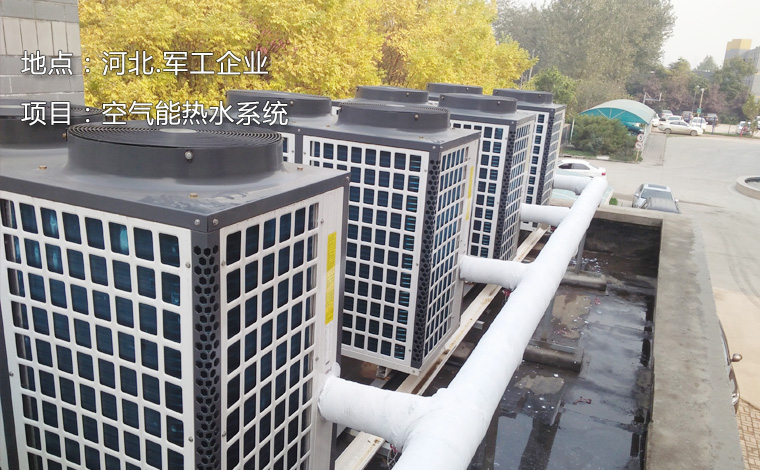
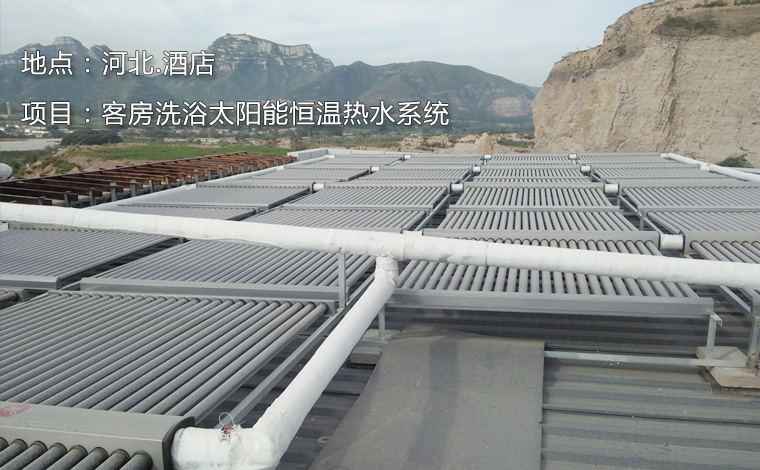
suncitygroup太阳新城官网是专业从事空气能冷暖系统、空气能取暖、空气能采暖,空气能太阳能系统、空气能系统、新风系统、净水系统及外围配套设施的研发、设计、销售、安装及维护服务的企业。公司研发了五大类型、三十多个品种的各类型产品。利用空气能太阳能节能方案设计,主要解决生活、工业、养殖、种植中需要的采暖、制冷、热水、恒温水等需求,涵盖范围涉及民用、商用、学校、医院、宾馆酒店、厂企、游泳场馆、足浴洗浴、工地项目部、工业加热、食品烘干和农业养殖、工业生产、部队等各场所。
公司通过ISO9001质量管理体系认证,公司拥有暖通工程师、热利用工程师、维修工程师等专业人才,是打造高品质工程的有力保障。
利尔佳公司致力于打造质量诚信品牌,沿着“做精、做大、做强”的战略方向,秉承“科技创新,携手未来”的观念,全力开发和推广绿色环保的空气能太阳能新能源产品设备;坚持品牌发展之路,以前瞻视野,做品质典范,创引未来,倾力为消费者提供稳定、高效、安全节能、环保健康的工程项目。
公司以高度负责认真的工作态度,严格的质量控制,星级的服务,广受用户好评。公司愿真诚与我们的客户一同致力于新能源的综合利用,共同呵护人类美好的家园。
suncitygroup太阳新城官网是专业从事空气能冷暖系统、空气能取暖、空气能太阳能系统、空气能采暖设备、净水系统及外围配套设施的研发、设计、销售、安装及维护服务的企业。
备案号:冀ICP备20000978号 冀公网安备13010402002808| 网站地图 XML地图
技术支持: